
GLP-1 receptor agonists are showing promise in areas beyond diabetes and weight loss, including potential benefits for cardiovascular health and reducing addictive behaviors. However, questions remain about long-term use, potential side effects, and the applicability of these findings to individuals living with HIV.
GLP-1 Receptor Agonists: Expanding Potential, Remaining Questions
Todd T. Brown, The Johns Hopkins University School of Medicine, Baltimore, MD, USA
The use of GLP-1 receptor agonists (GLP-1 RAs) has rapidly increased in the last five years, driven by strong data supporting their effectiveness in managing diabetes, cardiovascular disease, and obesity, as well as widespread discussion on social media. But is the enthusiasm surrounding these medications justified? Researchers are now working to pinpoint where the strongest evidence lies and identify key gaps in our understanding, particularly when considering their use in people living with HIV.
Recent presentations and studies have explored several key questions surrounding GLP-1 RAs.
- Could the ability of GLP-1 RAs to reduce “food addiction” be applied to other addictive behaviors? A small trial involving individuals with alcohol use disorder, detailed in Hendershot et al. JAMA Psychiatry, showed promising results in reducing alcohol and tobacco consumption.
- To what extent does the observed cardiovascular benefit stem from weight loss? Clinical trials suggest that only about 30% of the positive cardiovascular effects can be attributed to weight reduction alone.
- What impact do these medications have on cognitive function? While one meta-analysis indicated a potential benefit (Semminer, JAMA Neurology 2025), the EVOKE study, which investigated semaglutide in early-stage Alzheimer’s disease, did not demonstrate a significant effect on disease progression.
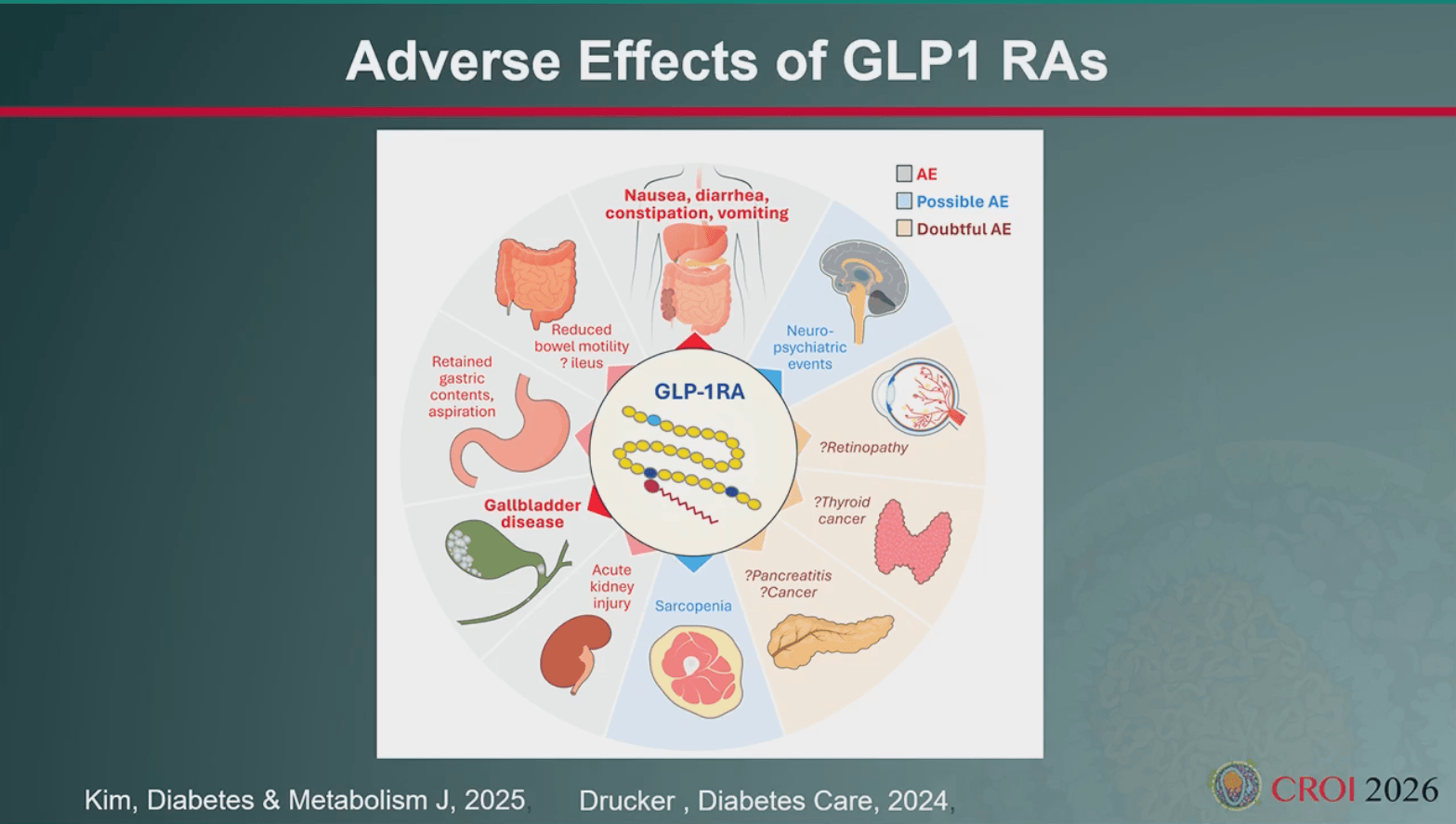
- Are the long-term side effects fully understood, and is there a risk of muscle loss (sarcopenia)? Data indicates a possible increased risk of fracture in the general population, along with a significant decrease in muscle mass – approximately 25% of observed weight loss is due to muscle reduction. Could these effects be more pronounced in people living with HIV? Some studies outside of registration trials have shown significant early discontinuation rates, with a median time to discontinuation of 1.4 years after starting treatment.
- Given their anti-inflammatory properties, could GLP-1 RAs have a specific effect on persistent inflammation associated with HIV? While data is still limited, preliminary studies (Furdenburg et al. OFID 2025) suggest a potential positive impact.
- How can the reversibility of effects upon treatment cessation be managed?
- Is the use of these medications safe for older adults? Despite considerable enthusiasm on social media portraying these drugs as “anti-aging” miracle cures, there is limited data available for individuals over the age of 75.
- Finally, questions remain regarding access, given the current costs and potential number of indications, and whether lifelong treatment should be considered, similar to HIV therapy, if the effects are fully reversible upon stopping the medication.
The substantial commercial activity surrounding GLP-1 RAs, generating billions of dollars in revenue for manufacturers, received limited attention during discussions. As the speaker noted, data should guide decisions, not simply enthusiasm. It’s important to remember that addressing the consequences of conditions like obesity shouldn’t overshadow the need to address the underlying causes, such as poverty and poor nutrition.
This article was originally published on the CoReSS Bretagne website and is reproduced here with the author’s permission.